
PCR Tests and COVID Vaccines are Useless
Home › Forums › The Automatic Earth Forum › PCR Tests and COVID Vaccines are Useless
- This topic has 45 replies, 23 voices, and was last updated 4 years, 3 months ago by
Dr. D.
-
AuthorPosts
-
December 3, 2020 at 4:30 am #66330
V. Arnold
ParticipantA classic false flag operation; everyone but “US” is involved.
Sowing fear and the consequent distrust in everything, is where we are now.
Control seems close to complete…
I’m doing my damnedest to not buy into any of “IT”.
At this time, Sputnik V is the only vaccine I would consider.
Thailand has opted for the two worst; Astra-zenica (sp?) & Pfizer…
Getting my D’s & C’s; and only listen to the news twice (morning/evening) a day; staying well clear of all print media except TAE.
Remember, fear is a thief; don’t let it steal from you…December 3, 2020 at 4:42 am #66331sumac.carol
ParticipantThank you to all who have contributed to this discussion and dug into the details and provided clarifications. As someone who has to get regular testing I am less concerned about what the test is doing. I also appreciate the info on the increase in total deaths in the US – was looking for updated figures (beyond the April figures shown earlier) but hadn’t found them.
December 3, 2020 at 10:22 am #66341CoolRunnerII
ParticipantOne control question to ask about PCR tests is: If you have a large false positive percentage, how can some areas have positive rates close to 0?
In my area in Norway we are at about 0.5% positive tests of about 6000 a week at the moment.
I would say that indicates that if there are no viruses going around, then there will be no positive tests. Or else the test that is used in Norway works differently from what is used by other countries.
December 3, 2020 at 1:43 pm #66347HerrWerner
ParticipantReally top-notch article, and commentary today in this entry. I’m sharing an article on accuracy of diagnostic tests I refer to often. These terms are specific to the medical profession, but statistics behind them are quite simple and this article explains it well: http://michaelandjudystouffer.com/judy/articles/specsen.htm
The TL;DR –
A test that is 97% accurate (which sounds terrific! and it is, high-90’s % represents the upper-bound of the best of medical tests) still results in significant false positives. In other words, your world sucks if you’re one of those 3% with a false positive. On top of that – and here’s the hard part – the accuracy of a test is specific to the population it applies to…The author explains this way: have a theoretical AIDS test with 99% accuracy – which is a very accurate test. Take 10,000 random people and test them with it.
* 99 people will really have AIDS and get a correct (positive) test results.
* One unlucky bloke will have it but get an incorrect (negative) test result.
Now the uninfected people?
* 9,801 will get a correct (negative) test result. Cool.
* 99 people will get an incorrect (false positive!) test result. Well, shit.
99 false positives, 99 people in the general population will be told they have AIDS when they don’t. And that’s with an unusually accurate test, with 99% specificity and sensitivity. I did a cursory search on the Interwebs and for the PCR test it has to be minimum 90% sensitivity and 95% specificity in the USA. UK is a bit higher. Not great compared to our theoretical 99% accurate test. And those figures are end-to-end performance of the test in ideal conditions, not the real-world of goofs, human errors, barely trained and tired HCP’s.Throwing a test like that at the general population with a (relatively) rare condition is foolish policy. The rarer the condition, the less accurate the test. That’s why before administering and AIDS test, other risk factors are considered (lifestyle, possible exposures, etc etc) These diagnostic tests deal with probabilities. You have to get to that subset of the population that is at risk before you roll the (fairly accurate) dice of the diagnostic test.
With COVID? The PCR test? Forget it. At least the way it is currently being used. You cannot estimate those risk factors like you can for that theoretical AIDS test. 11 months in, with the ‘Rona there are hardly any “risk factors” for exposure for the general public – it is ubiquitous in the population now. And still, as a percentage of population, relatively “rare.”
December 3, 2020 at 4:15 pm #66351madamski cafone
ParticipantSo an article says certain tests are useless for accurately telling if you have covid or not. The rebuttals to this reduce to equivocations that translate to ‘sometimes it is and sometimes it isn’t’. ‘It depends’, like John McCain’s infamous underwear.
In plain vernacular man on the street logic, the rebuttals lose. Plain vernacular man-on-the-street logic is how the public mind works.
Me, I think this whole silly squabble revolves around the unfortunate use of the word “absolute”, which is an emotionally satisfying word to use, and closer than not to accurate* when the hard facts of the data are related to the covid phenomenon, but also easy to dismiss because absolutes are ideals not realities. Even a subatomic particle is not absolutely one thing or another. It’s a phenomenon that follows a very narrow pattern in a fairly — but not absolutely — precise range.
Let me use more accurate language: the tests SUCK. Not absolutely but enough to be insufficiently useful to be worth messing with except, perhaps, as a stage of development in covid testing. It is the public who must trust and submit to testing for tests to be useful, and the public thinks “covid test” means, well, a test to see if you have covid. Period. How silly of them, right?
Oh, whatever shall we do when we run out of low-hanging fruit to pick on?
^%*
And I still have no patience with honorifics like M.D. in an egalitarian social setting. It’s one thing to tell us you’re a doctor. It’s another thing to use it as some kind of imprimatur or letterhead. If we were discussing gender/sex issues, it would be obnoxious if my handle were madamski, P.L. (Professional Lesbian). It’s enough to say I like vaginas when relevant to the conversation.
closer than not to accurate* like, allegedly, the tests currently under discussion.
December 3, 2020 at 4:43 pm #66356Dr. D
ParticipantAs far as I know, hospitals here don’t use PCR for exactly this reason: it doesn’t work worth a hoot. They don’t say that, they just say it “Doesn’t fit our needs” or some such.
Presumably they are using one of the many, many tests that DOES work, like Dr. Day says, and are able to get their feedstocks.
So…a year later, we have (many) tests that work and one test that doesn’t, and guess which one we’re using? And as noted, they are using both exactly as the inventor said not to, AND for a public-policy decision that it is illogical to use for.
How does this work? How in other nations/locations? They simply direct the labs to run 30x not 40x. Boom. “Cases” drop. Which some are suspecting they will suddenly “discover” there are too many false positives just about the day they release the vaccine, and reduce the number from 40, to 30, to 10, or wherever they like. Yay! Vaccine works a miracle! Profits rise!!! If the Gilet Jeunes give you lip, you just “Recommend” the labs in their areas move back to 40x. Boom. Instant lockdown til they’re dead and broke.
Meanwhile, hospitals, using a “better” test, i.e. one that works at all, are blissfully unaware, and all the medical Joes and Jeans remain compliant, and believing everything.
So Dr. or others, look at the chart: Deaths vs Cases.
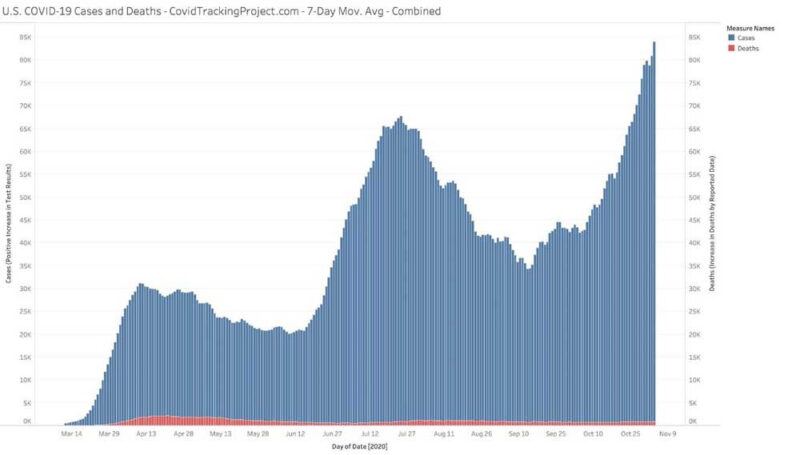
https://www.aier.org/wp-content/uploads/2020/11/casesdeaths-800×455.jpgIf it’s NOT true, then how do we have FEWER deaths than April? And the number of cases always rises, it’s now what, 200x the number of deaths? So your “testing” for “Cases” matches exactly my theory that people are tested, and the only way they think they have Covid — because no symptoms, no deaths — is from this false positive. …The one that will kill them slowly with grinding poverty and denied access to health screenings. We have a pandemic so bad nobody knows they have the disease without a test. Few people know anyone who’s died. Homeless and drug-addicted with compromised immune systems completely untouched, happily in a box, uninfected. Yes, that’s back to your “Gold Standard” problem, another whole kettle: not only can we statistically infer it’s 90% false positives (A Pfizer epidemiologist and statistician exec published an article on this in Britain I posted) but we can’t even calibrate it AGAINST a standard. (or just refused to)
Yes, this still leaves the door open for my theory to have other causes, but it’s not disproven in the least by a lot of squawking and handwaving. If anything, saying “Do as you’re told”/”I’m the expert” (That mis-reported H1N1, SARS, Avian, Swine, and eBola, approved AZT and Vioxx) tells me you’re all lying liars. You said no masks. You said 15 days. You said no transmission. You said 25 million dead. You said we were only going to slow it, not stop it. Wrong, wrong, wrong, wrong, wrong. So how about some humility when you’re dead dead wrong wrong for one year and running? I’ve been right the whole time and I’m some doofus living under a bridge, so clearly it’s not that hard. Dr. Day is neck-deep and he seems to be able to hit it right all the time, even with blackmailers circling like vultures.
So again, no additional death rate, and a disease so deadly no one can tell when they have it. Loss of all civil rights, apparently forever. Incredible, unimaginable increases in wealth for centralists, to the tune of multi-trillion$$, and a rushed vaccine that makes less medical and scientific sense than the disease. Now no Influenza deaths, no Heart Disease deaths. It’s a miracle cure! Que? Cui bono? You figure it out.
I’m going to go worry about things that are ACTUALLY dangerous. Like governments.
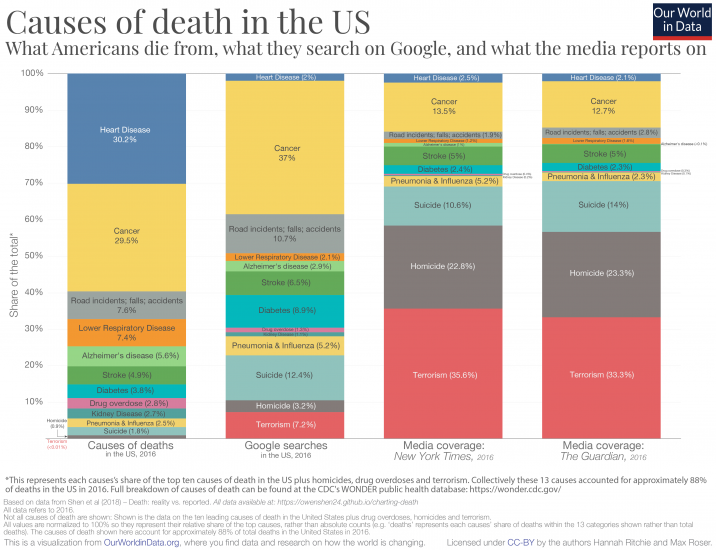
https://ourworldindata.org/uploads/2019/05/Causes-of-death-in-USA-vs.-media-coverage-716×550.png -
AuthorPosts
{kind=link}
{kind=link}
- You must be logged in to reply to this topic.
Sorry, the comment form is closed at this time.